AI-Powered Precision for Chemotherapy Benefit Prediction
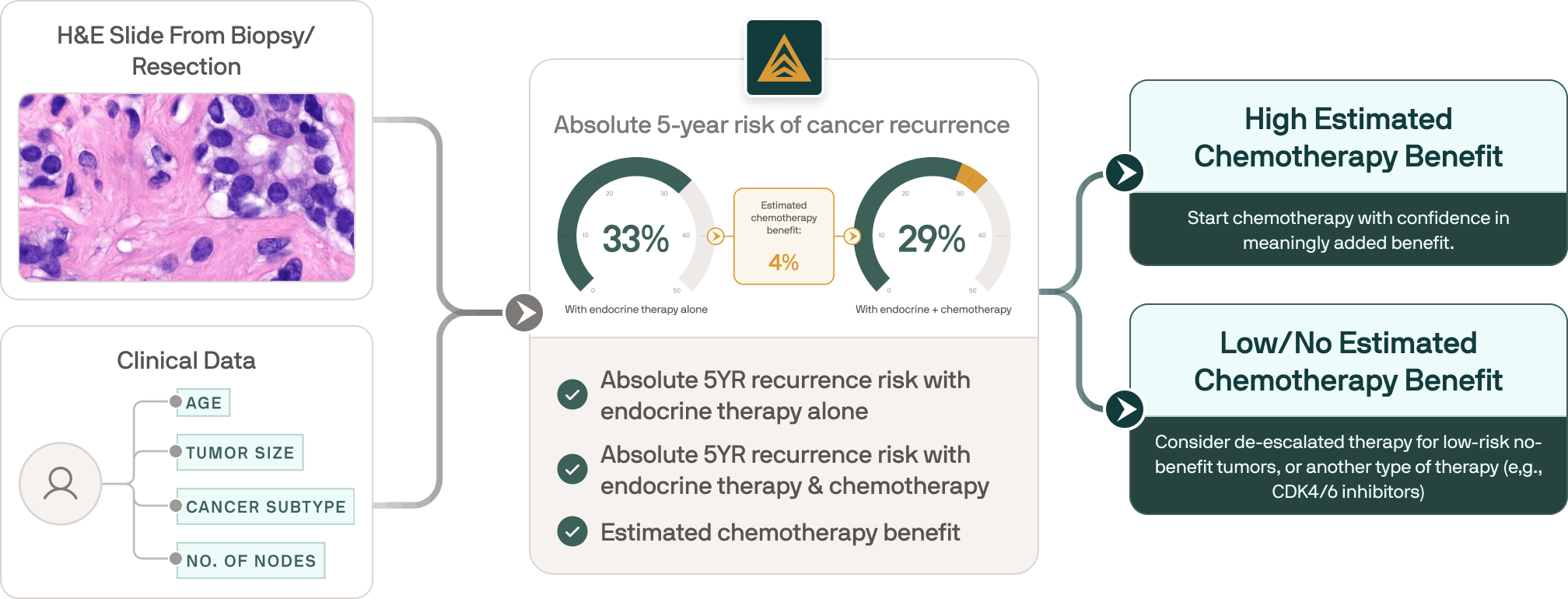
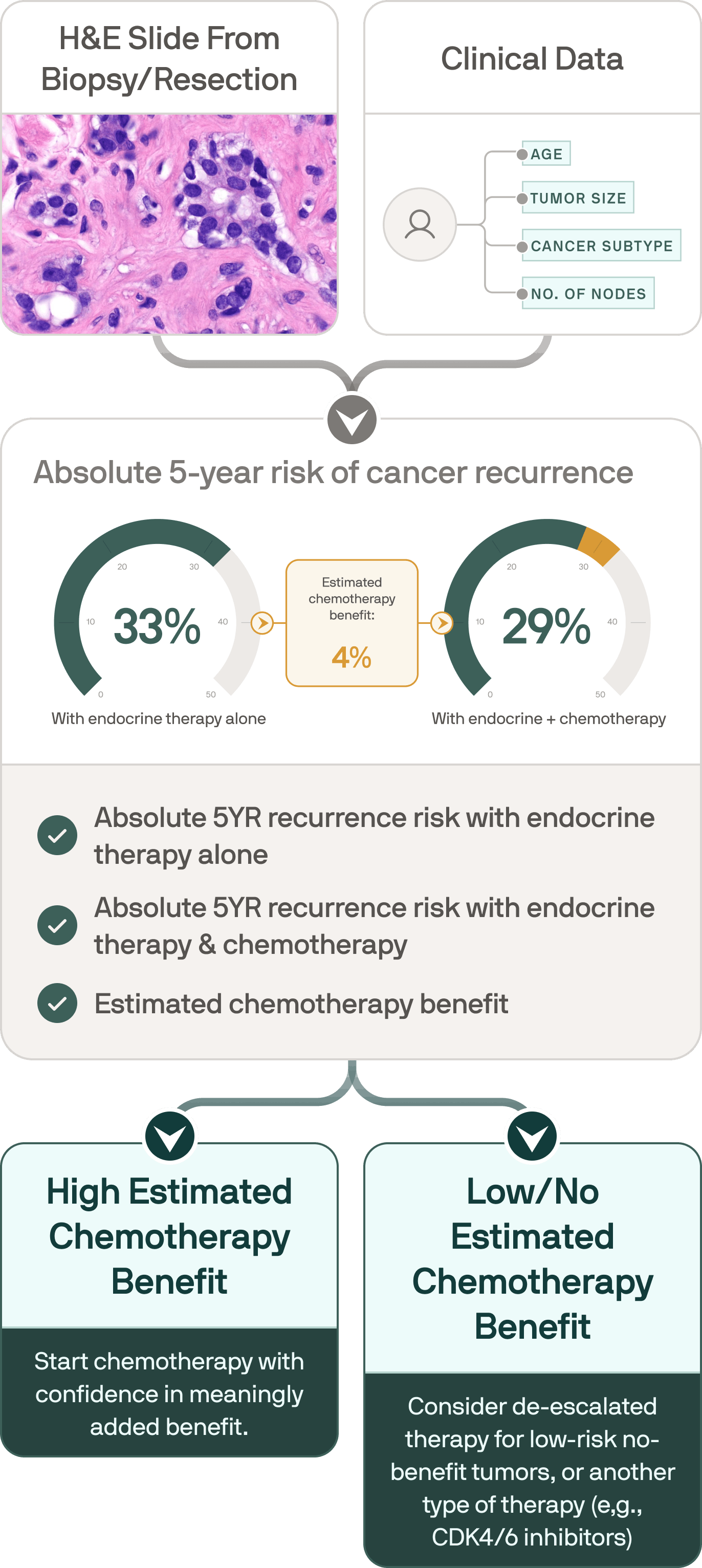
Beyond predicting recurrence risk, Ataraxis Breast quantifies individualized chemotherapy benefit for patients with early-stage HR+/HER2-negative breast cancer. By analyzing H&E slides and clinical data, it helps identify which patients are likely to benefit from chemotherapy and which may be unlikely to benefit, even when their recurrence risk is high.
Moving beyond population averages to provide personalized insight into chemotherapy benefit
Why individualized prediction matters
Choosing whether to add chemotherapy to endocrine therapy in HR+, HER2– early breast cancer is one of oncology’s hardest decisions. Most tools estimate recurrence risk or average group benefit, but not patient-specific chemotherapy effect.
Risk alone can mislead treatment decisions.
Real-world cohorts show the gap: about 1 in 4 “high-risk” patients is predicted to gain little from chemotherapy, while some “low-risk” patients may benefit substantially. This mismatch means some patients endure treatment with minimal personal benefit, while others who could benefit more are not readily identified. Ultimately, clinicians are left inferring individual decisions from population-level signals—an approach that falls short of true precision care.
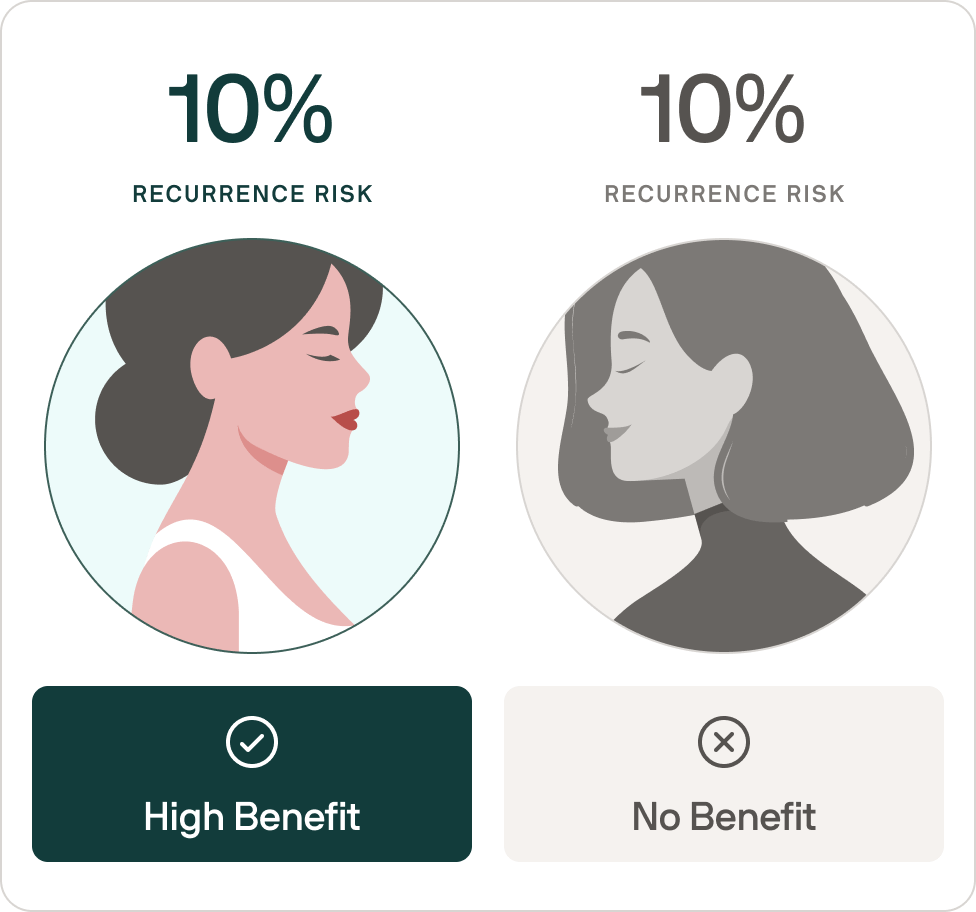
Same recurrence risk ≠ same chemotherapy benefit.
And that difference matters.
Know, for every patient, not averages.
Going beyond averages
.png)
.png)


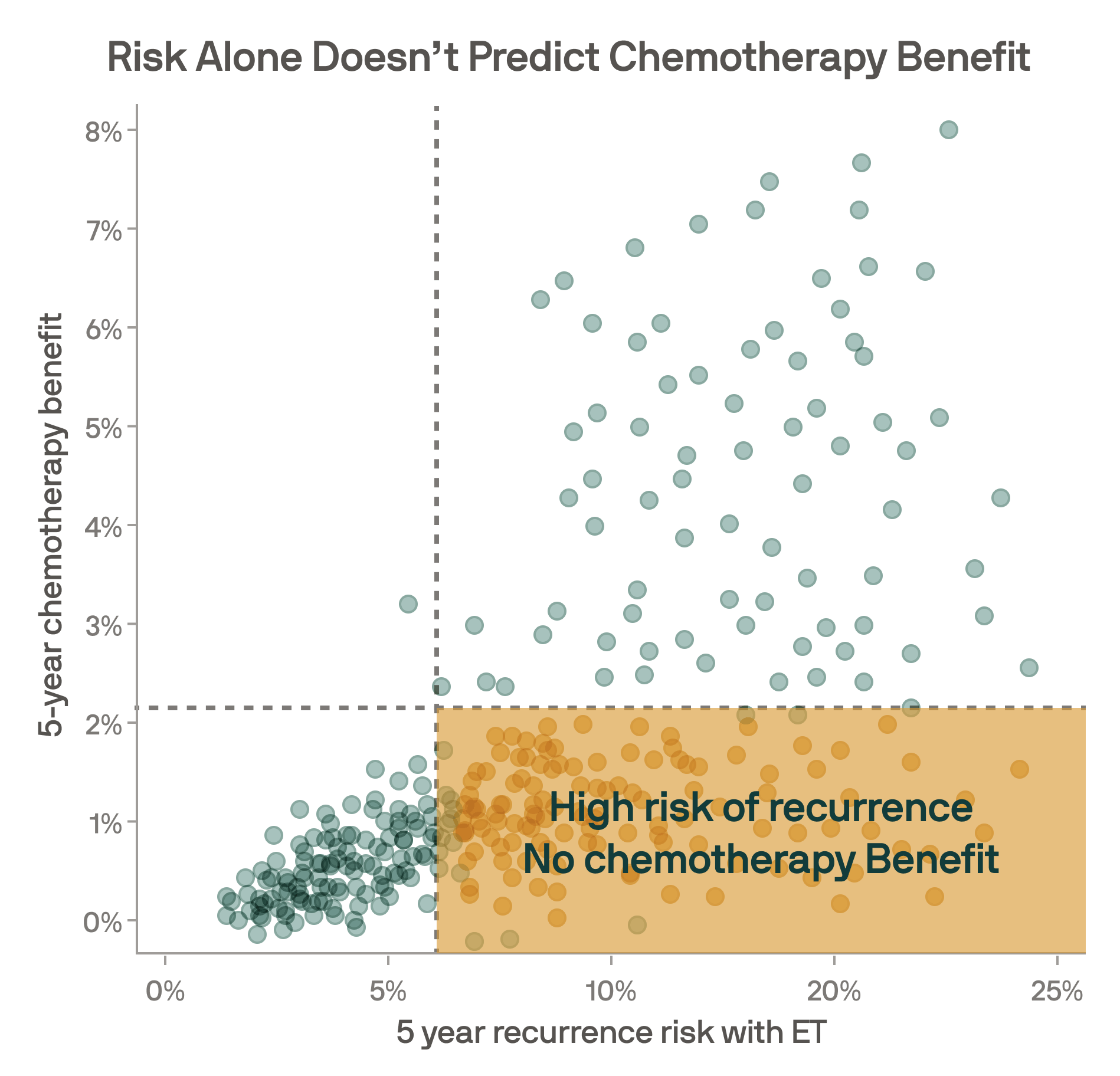
Reduce overtreatment. Identify non-benefiters.
Ataraxis finds high-risk patients with low/no chemotherapy benefit
22% of HR+/HER2- patients are high risk, but have less than 2% recurrence risk reduction with chemotherapy.
Patients with high risk of recurrence but low/no adjuvant chemotherapy benefit should be considered for other adjuvant systemic therapy options, such as CDK4/6 inhibitors.
Clinical application of our test

Ataraxis Breast can identify and quantify estimated chemotherapy benefit in all HR+ HER2- patients, regardless of their risk of recurrence. Then, depending on your and patient’s preferences, identify patients who should receive adjuvant chemotherapy.

Patients with high risk of recurrence but low or no benefit from adjuvant chemotherapy might be considered for appropriate treatment strategies such as adjuvant CDK4/6 inhibitors, ovarian function suppression, PARP inhibitors, and SERDs, improving alignment between biology and therapy.

Find patients with low or no predicted chemotherapy benefit, including those with high recurrence risk by traditional genomic assays, and confidently spare them unnecessary toxicity and cost.
How do we predict chemotherapy benefit?
In ER+ HER2- patients, Ataraxis Breast identifies patients who benefit from adjuvant chemotherapy
Predicted high benefit group (n=191)
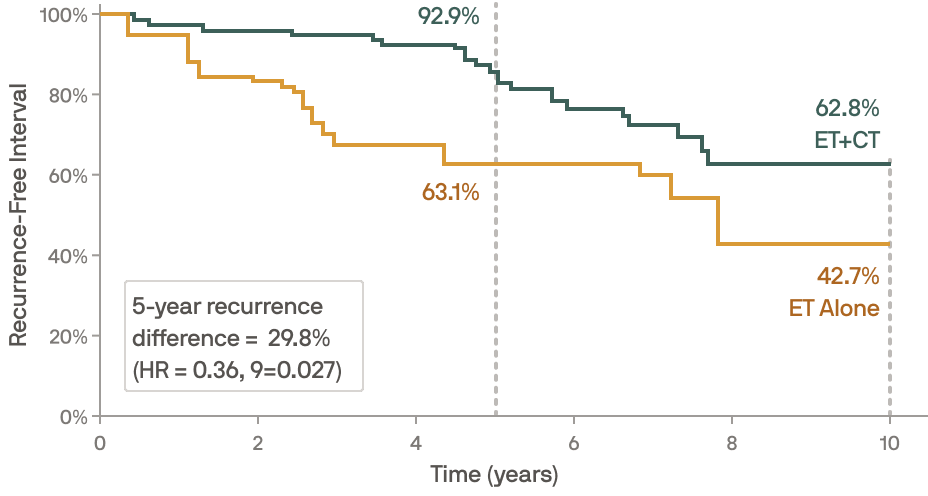
Predicted low benefit group (n=1339)
.png)
Learn more about our technology
Make the most informed call for your patients.
What if you could know how much chemotherapy affects your recurrence risk?
For many years, chemotherapy recommendations have relied on how large groups of patients responded on average—not on how you as an individual might respond. That’s why many people focus on a single risk score or cutoff (i.e., “my risk score is X, so I don’t need chemo”). But two people with the same score can experience very different benefit from chemotherapy. Traditional tools can tell you whether your overall risk of recurrence is high or low, but they can’t show whether chemotherapy is actually likely to move that risk in a meaningful way.
Same recurrence risk ≠ same chemotherapy benefit.
And that difference matters.
Know, for every patient, not averages.
Risk alone can mislead treatment decisions.
Real-world studies reveal a gap: about 1 in 4 people labeled “high risk” may be expected to get little benefit from chemotherapy, while some labeled “low risk” could benefit a lot. This mismatch can mean some patients go through chemotherapy’s side effects with minimal added help, while others who might benefit most aren’t clearly identified.
Understand your likelihood of benefit—not a one-size-fits-all risk label
Using the same pathology slides already collected during your care, Ataraxis Breast estimates your personal benefit from adding chemotherapy to endocrine therapy. Instead of placing you into a broad risk category, our test shows quantifiable percentage reduction in recurrence that chemotherapy is expected to offer for you specifically.
Your doctor can use this information to:
How do we predict chemotherapy benefit?
Going beyond averages